Is it possible that those personality traits and characteristics associated with “being feminine” are, in themselves, depressogenic? Isn’t it true that the line between “neurotic” dependency and “normally higher” feminine dependency needs is a difficult one to draw? It may be that being “normal” and being “normally feminine” might not be quite the same thing. I want to talk now about the witty (if somewhat devastating in their implications) researches carried out by Inge and Donald Broverman and their colleagues. This work was reported upon in the Journal of Consulting and Clinical Psychology in 1970.
What the Broverman group did was to devise a deceptively simple list, a brief questionnaire, in which a number of traits considered highly feminine were placed on a scale of I to 10 with their “masculine” opposites at the other pole. The Broverman list looked like this:
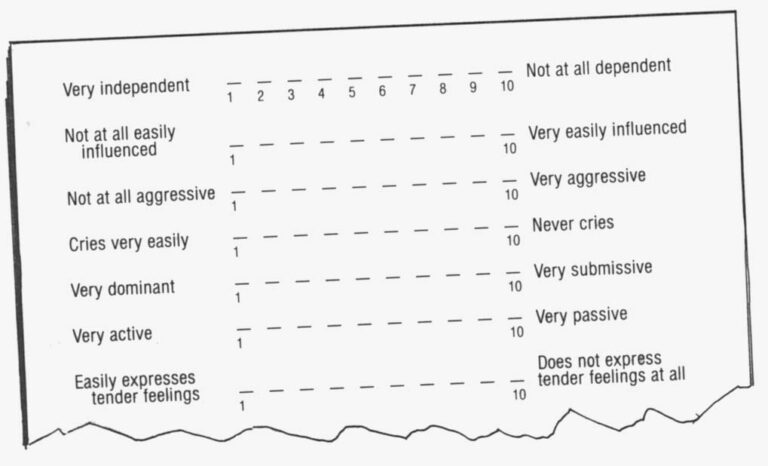
And so forth…there were 38 such masculine” – ” feminine” personality traits placed in contraposition to one another on the Broverman questionnaire.
The researchers then sent this sheet around to three different groups of psychotherapists, with three different sets of instructions. The first group of clinicians was asked to describe the “mature, healthy, socially competent woman”-by checking the places, on this scale of normal personality traits, where she would most obviously fall-and the second group was asked to “think of normal, adult men and then indicate on each item the pole to which a mature, healthy, socially competent man would be closer.” The third set of psychotherapist-subjects was asked, simply, to describe the “healthy, mature, socially competent adult.” In this last set of instructions, no sex was specified.
The three groups to which the questionnaire was sent were roughly similar in composition-they included psychologists, psychiatrists, psychiatric social workers, of whom slightly less than half were female, slightly more than half, male. When their findings were analyzed, the Broverman workers discovered (to no-one’s surprise) that the personality-trait-profile of the “healthy adult female” looked very different from that of the “healthy adult male.” On an item, for example, such as “Does not hide emotions at all” on the low-numbered side, which is opposed to “Almost always hides emotions” on the high side, “healthy males” were perceived as falling in the 7 or 8 to 10 range, while “healthy females” were down at the 1 to 4 end of the scale. This might, of course, be seen as merely a way of rephrasing the obvious: We all know that the feminine sex-role leans towards, or one might say “prescribes” more emotional expressivity. And if adjustment to social norms is considered to be a part of mental health, the woman who conforms to and is at peace with the pressure of these expectations, ought to be someone “healthier.” Her higher level of emotionality is appropriately feminine.
Nevertheless, as Broverman et al noted, an examination of the overall content of the items, and the ways in which the clinicians responded to them, “conceals a powerful, negative assessment of women.” On the face of it, there would seem to be nothing odd about the fact that these psychotherapists expected to see more traits that are stereotypically masculine in the “mentally healthy adult male”: nor is it strange that the “healthy female” was expected to display stereotypically feminine traits. “However,” observed the Broverman researchers, in their report,”…clinicians are more likely to suggest that healthy women differ from healthy men by being more submissive, less independent, less adventurous, more easily influenced, less aggressive, less competitive, more excitable in minor crises, having their feelings more easily hurt, being more emotional, more conceited about their appearance, less objective, and disliking math and science. This constellation seems a most unusual way of describing any mature, healthy individual.”
The difference in the description of the “healthy male” and the “healthy female” wasn’t, however, the real kicker in the Broverman study. Their most ludicrous result had to do with that third category-the “healthy, mature, socially competent adult,” no sex specified. For this “healthy adult” turned out-when the three groups of answers were compared-to be completely indistinguishable from the “healthy adult male.”
Abstract notions about what is “mentally healthy” (as long as sex isn’t mentioned) seem to emphasize those “masculine” traits and characteristics that are more prized, more valued in our society. The lesser status, less-valued “feminine” personality traits-less aggression, less dominance, more freedom of emotional expression, more excitability, etc.-were not seen as consonant with emotional well-being in the adult individual, sex unspecified.
As far as a general standard of mental health is concerned, the feminine role apparently implies pathology!
As the Broverman researchers put it: “For a woman to be healthy, from an adjustment viewpoint, she must adjust to and accept the behavioral norms for her sex, even though these behaviors are considered to be less healthy …(This) places women in the conflictual position of having to decide whether to exhibit those positive characteristics considered desirable for men and adults, and thus have their “femininity” questioned, that is, be deviant in terms of being a woman; or to behave in the prescribed feminine manner, accept second-class adult status….” The problem is, in brief, that women who display those more masculine, “healthier” personality traits-competitiveness, ambitiousness, adventurousness, who are “not at all interested in own appearance,” and who are aggressive and assertive-lay themselves open to the subtle but deeply punishing accusation that they aren’t “feminine.”
Terri Funabashi is a beautiful, second-generation Japanese-American woman who is now a third-year resident in psychiatry at a major university affiliated crisis-clinic. Terri volunteered to be interviewed for my “women and depression” study. I remember being taken aback. She wasn’t, by any means, the first female psychotherapist to offer herself as “subject, ” but she did seem so quietly in command of most situations, so self-assured, so composed. “Are you depressed enough to qualify?” I asked with a smile, looking at her inquiringly.
“Isn’t everyone?” she replied lightly.
Later, during the course of our taped conversations, Terri told me of an incident, which, she said, had plunged her into a “raging funk” for most of the fall semester of the previous year. She’d been a new M.D. then, spanking fresh out of medical school, and beginning her psychiatric residency at a major university affiliated hospital. But she wasn’t, as she phrased it, “paying too much attention to what I wore, to clothes, to that sort of thing. I mean, she explained, “I was always neat, and whatever I had on was clean-but I really wasn’t paying a whole lot of attention…” About six weeks after the term had started, related Terri, she’d been having coffee in the residents’ lounge with six or seven of her colleagues (all male), when the discussion of a particular woman patient had arisen.
“This woman had been hospitalized, with a severe depression, on the in-patient unit Terri told me. “She was a very passive, very dependent person who was in a marriage with a dominant, aggressive, bullying kind of a husband. And part of the problem was, we felt, the fact that she was out of touch with her anger. We all believe she was sitting on some pretty violent rebellious reactions-and turning them in upon herself,’ because it was too psychologically threatening to experience them in relation to her husband, whom she needed.” The patient’s unacknowledged fury was, everyone agreed, at the core of the depressive reaction. But Terri, her primary therapist, had been (thus far) unable to help her to organize her anger, to make an assertive squeak in her own behalf. “I can’t understand it,” she’d complained, during this impromptu conference.
To which one of her fellow Residents had replied off-handedly: “That’s because you yourself are not very feminine.”
No-one else present, said Terri, had seemed to respond to this statement at all; it was as if her colleague had mentioned the weather, or some other relatively unequivocal matter of fact. The conversation had continued, and she’d managed to maintain her own part in it-inwardly, she’d felt gutted, assaulted, devastated. Even now, over a year later, her eyes widened, started forward in her face with the remembered shock. She leaned backwards in her black leather easy chair, as if physically pushed there by the remembered impact of those words.
We talked then, about the thinly disguised hostility, the putting-her-into-her-place impulse that had triggered his cruelly “objective” comment. What, about Terri, had aroused his own anxiety-what had made him want to strike out at her in that way? I asked about whether or not she’d been, at that time, a “free” female, i.e., potentially available as date, as possible lover …? She shook her head “No” at once. She’d been living with someone, a fellow doctor, a man whom she was now engaged to marry. I wondered, aloud, whether the fact that her male colleague seemed to want to devalue and punish her might have had something to do with his feeling some attraction for her. I laughed, made some remark about the “sour grapes response.” (In her 1932 essay on “The Dread of Woman,” Dr. Karen Homey observed that: “According to my experience, the dread of being rejected and derided is a typical ingredient in the analysis of every man, no matter what his mentality or the structure of his neurosis.” The need of men, as a group, to disparage women, as a group, is, suggests Homey, based upon “a definite psychic trend …a tendency rooted in the man’s psychic reactions to certain given biological facts, as might be expected of a mental attitude at once so widespread and so obstinately maintained. The view that women are infantile and emotional creatures, and as such, incapable of responsibility and independence, is the work of the masculine tendency to lower women’s self-respect.” But what really counts here, and what really is at stake, writes the psychoanalyst, is “the ever-precarious self-respect of the ‘average man’….”)
Terri’s fellow doctor had, undoubtedly, been disturbed by her failure to be;”womanly” in the way that he understood womanliness. ” She’d failed to conform to the stereotypic blueprint for female behavior insofar as dependence, submissiveness, emotionality, and other traits, of the “healthy adult female” (such as low degree of competitiveness, high interest in self-adornment, etc.) were concerned. To be truly feminine, Terry would have had to preoccupy herself more with the kinds of clothing she wore, with making herself more attractive. In the meanwhile (so went her colleague’s message) he wouldn’t be sexually interested in her even if she happened to be available because she was unfeminine. And this puts at rest any unspoken, underlying, perhaps never even consciously thought about issues relating to who might be rejecting whom. He had retained his own sense of self-esteem and command of the situation…if at some cost to Terri.
For what was evident was that now, almost two years later, the competent young Dr. Terri Funabashi, a third year resident in psychiatry at one of the country’s foremost medical schools, still carried that remark around like a piece of psychological shrapnel that was always capable of “acting up.”
And it did so, every once in a while. It gave her pain, and she did things to avoid that pain-had “changed” in order to do so. Perfectly capable, at this moment, of understanding what his own needs and motivations might have been, and the essential humor of his entire ploy, Terri still had-and in the midst of our conversation-done a sudden turnabout.
“Of course,” she’d told me, leaning forward and speaking in a voice that picked up speed as she plunged off in a reverse direction, “I did wear my hair differently at that time; I wore it back in a bun. Now,” she explained quickly, picking up a glossy black hank as if to underscore what she was saying, ” I wear it loose …And my shoes,” she went on, raising one foot slightly to show me her stylish maroon leather wedgie sandals, “are different too; I used to wear just those Wallabees, you know, whatever was most comfortable and practical.”
She was being a good “feminine” girl now: That offhand remark had shot straight to a vulnerable place in her psyche. It had traveled straight to the issue of her sexual identity, the core question of whether or not she was fully and successfully a woman. And she’d shifted, in response to this incident, on at least two of the items in the Broverman questionnaire. She’d moved from the more masculine “Not at all interested in own appearance” and in the direction of the more feminine “Very interested in own appearance.”
She’d shifted, too, on a very similar, if more harshly worded item. She’d gone from “Never conceited about appearance” towards “Very conceited about appearance” as well.
Now, a lack of great concern about appearance had been, on the profile of the “healthy, competent adult” one of the earmarks of general psychological well being. That is, if the sex were unspecified. So Terry was, according to this standard, less “mentally healthy.” She was, however, more “feminine” in certain of her attitudes, her behaviors; she was more like the stereotypic view of the “healthy, competent adult female.”
The dilemma was that being a “healthy adult” and a “healthy female adult” were difficult tasks to reconcile. They weren’t really the same thing, not at all. And in fact some of the symptoms of depressed states for example, “Cries very easily,” “Feelings easily hurt”-were viewed, when they appeared on the Broverman questionnaire, as aspects of normal femininity. So were “Very submissive,” “Very passive,” “Has difficulty making decisions” considered traits that fell within the “healthy female adult” spectrum. Some of these are, in fact, outright symptoms of depression (for instance, difficulty in making decisions is one) or are a hair’s breadth away from them. (Submissiveness and passivity are not terribly distinct from the psychological symptom of “Feelings of helplessness and powerlessness”.)
I’m not, of course, suggesting that the normally feminine adult is a depressed person. I just want to raise the possibility that the yellow brick road that she follows throughout the course of her life-cycle may be bordered by many more depressive gullies and potential “falling-off-places” than is the case for her “Healthy, socially competent” male contemporary.
©1979 Maggie Scarf
MAGGIE SCARF is spending her Fellowship year studying depression among women.